
A simple legal record or captivating puzzle pieces? Many therapists and counselors put off writing their formal notes, especially when they’re busy with clients. Just like we ask our clients to reframe, perhaps you can too? The more you see your therapy notes as a tool in the process, the more beneficial they’ll be for everyone.
While therapy notes are a legal requirement, they also offer therapists an opportunity to reflect. As you formulate each client case, you can use these notes as a framework to guide your thinking.
It’s much easier to gauge if the course of treatment suits the symptoms and root cause when everything is clearly written down. In short, therapy notes give you the big picture overview as well as acting as mile markers for your clients’ journeys.
Most importantly, all therapy notes need to be HIPAA compliant if you’re operating in the US and GDPR for Europe and worldwide. Although, as we’ll see, your own personal psychotherapy notes aren’t covered by the regulation.
Either way, all the information you need for therapy notes can be safely and easily recorded with a platform like Quenza. It’s both HIPAA and GDPR compliant so you don’t have to worry as the templates are ready for you to use.
Moreover, you get access to a large library of worksheets, exercises, visualizations and more that you can put together into client journeys. These will also be recorded online under each client’s portal.
Why not see for yourself by signing up for the free, full-access, one-month trial? The activities will transform your clients’ experience and the headache of documentation logistics will be taken care of.
Understanding Therapy Notes
Understanding what are therapy notes means first defining psychotherapy notes. While the words are often used interchangeably, therapists need to understand that psychotherapy notes are not tied to privacy regulations.
The official definition of psychotherapy notes is that they are the therapist’s personal notes. These include any thoughts that could help them analyze the case.
On the other hand, therapy notes that need to follow HIPAA and GDPR rules include anything that relates to any prescriptions or interventions that have been used. They also contain any diagnostics, treatment plans, symptoms and progress [1].
In more general terms, therapy notes complement a client’s medical records because of the blend of objective and subjective interpretation that they provide. As counselor Dr. Rhonda Sutton who wrote the book The Counselor’s STEPS for Progress Notes alludes to, they are the puzzle pieces you need to “crack the case”, just like any good detective [2].
More specifically, therapy notes are both legal record-keeping tools as well as a way of tracking progress and responses to interventions used. In other words, through their therapy notes, therapists test and fine tune their hypotheses to offer the best treatment possible.
Types of Therapy Notes
To appreciate the benefit of writing notes, we need to define the different types of therapy notes. We’ve already briefly mentioned psychotherapy notes but the table below gives a more detailed overview.
|
|
Purpose
|
Format (To be explained below) |
|---|---|---|
|
Progress Notes
|
Systematic record of the needs and type of therapy a client needs throughout the journey
[2].
|
There are different types of progress notes with acronyms for each: |
|
Process or Psychotherapy Notes
|
Private reflections that are protected from regulations. The aim is to enable therapists in their case formulation.
|
Free form
|
|
Intake Notes
|
To provide an overview of the client’s situation, needs and wants at the first session.
|
Structured format to include background, referral notes where relevant as well as the presenting problem, strengths, issues and goals.
|
It can be difficult to know what can go into process notes while still following regulations. A good way to think about this is to remember that all facts and conclusions need to be in the progress notes. On the flip side, your own notes can include how you feel about the client. You might also want to remind yourself to refer to something before the next session.
Then, what are intake notes? Yes, they sound similar but they’re essentially a snapshot taken at the first session. They’re also an opportunity to engage with the client in the form of onboarding. So, be sensitive to the best way to send your client their forms.
Career Counseling Intake Form

With Quenza, you can onboard clients into the platform with their very own dashboard. They’ll be able to easily access their forms. Moreover, they can quickly access and read any supporting information you send them. For instance, it’s best practice to explain why you’re asking for their information and which regulations you follow. This helps them understand their rights as well as starting to build a rapport.
Overall, writing clear and systematic notes will help you become a better therapist or counselor. You’ll be able to use them to see the big picture, tweak your interventions when needed and generally optimize your strategies [2]. Reading our article on how to incorporate a Therapy Note System in your practice might also be of interest to you.
Confidentiality in Therapy Notes
In summary, what are therapy notes? They are clearly structured documentation that holds all the medical information pertaining to a client. They also include details about the treatment and how the responses are meeting a client’s goals.
With all that in mind, are therapy notes confidential? Yes!
Even process or psychotherapy notes need to be confidential. As explained, progress notes are governed by privacy and security rules within the US HIPAA or European GDPR.
Many therapists ensure they follow both regulations to be safe. It’s worth noting that GDPR doesn’t just cover Europeans. It also covers Europeans no matter where they reside. So, you need to make sure that your notes can’t be disclosed to anyone without your clients’ permission. Although, there are some legal exceptions and situations when the duty of care to the public becomes the greater concern.
When it comes to confidentiality, you need to think beyond just your therapy notes. Explaining confidentiality and its limits to your clients is another way to engage and build trust with them initially. Without confidentiality in therapy, your clients wouldn’t open up and nor would they know how to manage their own information about their therapy.
Learning to Observe and Writing Therapy Notes
When reviewing the types of therapy notes, the critical one that needs to be systematically written is the progress note. It’s an important skill to develop because it means you don’t forget anything while having the stepping stones to recovery for your clients.
Having said that, knowing how to write therapy notes isn’t always easy. How much detail should you include? In fact, what does “attention and detail” mean in practice?
To make things easier for therapists and counselors, the following acronyms were developed to provide a framework for the information. You’ll notice the last one is a proprietary approach developed by counselor Dr. Rhonda Sutton who also struggled for years to write progress notes that helped her make a difference for her clients.
Overview of the Types of Therapy Note Frameworks
|
|
Structure
|
Overview
|
|---|---|---|
|
SOAP
|
Situation, Objective, Assessment, Plan
|
A comprehensive framework that allows therapists to differentiate between subjective and objective observations
|
|
BIRP
|
Behavior, Intervention, Response, Plan
|
An easy-to-use process that focuses on behaviors to get to the depth of the root cause.
|
|
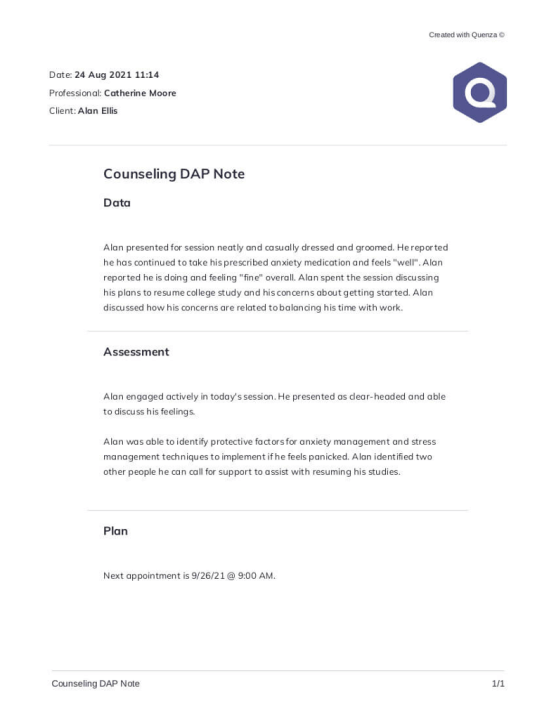
DAP
|
Description, Assessment, Plan
|
A useful overview for cases that don’t have many medical notes that need to be kept separate.
|
|
GIRP
|
Goal, Intervention, Response, Plan
|
A goal-focused framework that refocuses clients away from problems and into a can-do goal driven mindset.
|
|
STEPNoteTM
|
Subject & Systems, Tools (interventions), Evaluation, Plan
|
An alternative framework with a detailed book containing case studies that can act as a reference if needed.
|
One of the commonest mistakes whenwriting progress notes is not being precise enough. This takes practice. To help you, there are two wonderful exercises in the book The OTA’s Guide to Documentation [3].
The first exercise asks you to observe someone making an object, perhaps out of clay or with some arts and crafts. You then list 10 or more skills and factors you observe.
The second exercise is similar but this time, you’re watching someone prepare a dish. It can be as simple as breakfast cereal. The point is to describe what you observe without making assumptions.
How to Use Therapy Notes
Now that you know how to write therapy notes, it’s time to use them to your advantage. They essentially become your roadmap that details both the direction and the blocks to maneuver through. While all therapists enjoy face-to-face time with clients, these notes allow practitioners to evaluate their approach and track progress [2].
We’re all rushed off our feet but the sooner you write the therapy notes, the more insightful and accurate they will be. You’ll be able to fully define a client’s mood, responses and general functioning with all the details you need [3].
While it might be tempting to use abbreviations or to jump straight to conclusions, it’s critical to note the full process. So, instead of writing “client seen for depression”, it’s better to write “client is overcome with negative thoughts, can’t sleep and is struggling to get out of bed in the mornings”.
Furthermore, this provides valuable information of the complete journey for any colleagues should a client need to be referred. Increasingly, healthcare providers are collaborating to provide holistic care. The better your therapy notes, the better your clients get cared for.
Empowering Your Clients with Therapy Notes
As you can imagine, it’s critical for you to know how to document therapy notes. As we’ve mentioned they need to be clear and precise. Any issues that come up during therapy or potential risk to the client should be included.
Writing your therapy notes as soon as possible after sessions also gives you a chance to think ahead. In a sense, they serve as pre-planning before your next session. As you reflect, you might also think of other exercises that the client could benefit from.
For example, your client originally came in for anxiety but you’ve already uncovered unresolved grief. Could something else be going on?
Working Through the Four Tasks of Mourning

Coping Styles Formulation

It’s worth noting a more recent development in the world of progress notes. As part of the 21st Century Cures Act in the US, the “Open Notes Rule” has been active since April 2021. The aim is to increase client engagement and autonomy [4].
Many practitioners had already naturally adopted this practice because it increases client trust. After all, the notes are about them and therapists want them to take ownership of their health and well-being. By reducing the “doctor knows best” assumption, open notes can only deepen the therapeutic alliance [5].
Naturally, how open notes are shared with clients depends on the situation and their mental state. If you remember though that progress notes are not judgements but factual observations and subjective conclusions based on fact, it’s easier to see how clients could, and should, read them.
Furthermore, the research shows that despite therapists’ fears that open notes will create confusion, they have actually promoted client empowerment [5].
Who Can Request Therapy Notes
When you know who might end up reading them, it’s easier to consider how to document therapy notes. We all know that we write differently when we’re aware that someone else will read our words. In addition, we wouldn’t want clients to misinterpret their therapy notes.
In terms of who can request therapy notes, clients, or their legal guardians, are the only ones under the HIPAA and GDPR regulations. However, there are legal exceptions when therapists are given a court order.
Additionally, if a therapist deems that either the client is at risk of harm, or someone around them, they have a duty of care to consider who to inform. For more information on this, read one of our previous blogs on understanding client confidentiality.
Finally, many insurance companies can ask to see progress notes where patients are making claims for their therapy. Generally, clients sign a consent form so this will happen without necessarily being informed.
Even without the consent form, progress notes are handed over to insurance companies to allow them to determine how to pay any claims. Psychotherapy notes, though, will never be disclosed and are always protected as fully confidential from anyone except the therapist who wrote them.
Understanding Intake Notes
So, are therapy notes confidential? Yes, they are but between you and the client. As such, clients have every right to request them and ask for them. It’s therefore a sensible approach to always keep that in mind when writing your therapy notes.
Another point to note when reviewing who can request therapy notes is to remember guardians. Some clients are under care either because of their age or their mental state.
All these points apply when creating and storing intake notes. As we described in our article on therapy intake forms, there are 5 key sections to include:
• Patient data (name, contact, etc.)
• Insurance information
• Medical history (including mental health)
• Symptoms, and
• Desired outcomes.
Couples Counseling Intake Form

Overall, what are intake notes and why are they important? They set the foundations for a successful therapy journey. With these forms, you know your clients’ contact preferences and current situation.
Some intake forms also include medical history and a brief overview of financials, relationships and living arrangements. The idea is to gain a holistic view of your clients to better understand their presenting problems and goals, also noted on the intake form. You now have a baseline to compare to as you move forwards with the therapy journey.
The Nitty Gritty of Progress Notes
Now we know how to answer the question “what are progress notes”, let’s get into the details. While regulations cover how the information is handled, there isn’t always formal legislation or guidelines for how progress notes should be written.
However, keep in mind that your accreditation or licensing body, employer, or the payer of your client’s account (if not the client themselves) may have requirements of what needs to be included in progress notes.
To give you a starting point, the basics should include at least the following [2]:
• Name of client
• Session date
• Session length
• Type – whether individual, couple, family or group
• Where the session took place or if it was online
• Details about how the client presented themselves along with the presenting problem
• Particulars of what was said, including a list of the major topics and themes
• Any therapeutic activities or interventions undertaken
• An assessment of the client’s level of functioning
• Progress when compared to the goal or the treatment plan
• DSM code where applicable
• Signed and dated by the therapist or counselor
As previously mentioned, there are also different types of progress notes but we’ll see those details in the next section. Regardless of which type you use, they enable you to record an overview of the therapeutic interventions, along with a way to track progress and overall change.
Writing the Best Types of Progress Notes
While each of the frameworks for writing progress notes is similar, here are some tips for each one.
• SOAP Notes (Situation, Objective, Assessment, Plan). A useful tip for remembering to cover everything when detailing the situation is to use the acronym OLD CHARTS. In other words: Onset, Location, Duration, Characteristic, Alleviating & Aggravating factors, Radiating or Relieving factors, Timing, Severity [6].

• BIRP Notes (Behaviour, Intervention, Response, Plan). While SOAP is more about noting the facts, BIRP notes focus on the tone and mood of the session. Therapists simply observe the behaviors without judgment.

• DAP Notes (Description, Assessment, Plan). Just like for SOAP and BIRP notes, make sure you keep your sentences succinct. For this one, you also need to gauge what information to include in the Description that is relevant to the client and their presenting problem. As it combines the S and O from SOAP into one, your D in this case can be simpler but it has to match the client’s needs.
• GIRP (Goal, Intervention, Response, Plan). This framework starts with the goal which gives you a unique angle from which to work. Rather than focusing on problems, you’re driving the client forward with a positive and proactive approach. To discover more, don’t miss our comprehensive guide on GIRP notes.
Make Your Therapy Notes Count
Overall, therapy notes are either progress or process notes, sometimes referred to as psychotherapy notes. The latter are a therapist’s private notes but the former are a legal record. In a sense, you can also answer the question “what are progress notes” by saying that they form the map of the therapy journey.
Therapists and counselors who write concise and timely therapy notes leverage them for reflection and forward planning. These aren’t just notes to hide in a drawer or in a folder. They become active milestones that track progress. Moreover, now that open notes are actively being encouraged, especially in the US, clients can further use them to gain ownership over their therapy.
The use of open notes is even more applicable in today’s digital world. Essentially, clients can access these on their Quenza portal, for instance, and use them to reflect. They can then proactively send their questions through the chat function and feel more motivated to complete their homework.
Just like therapy notes give therapists the big picture, so clients also see where they’re going. It makes the hard work much more doable if you can see the goal. So, focus on getting the right therapy notes in place and use them as living documents to drive more sustained and longer-lasting change with your clients.
See this for yourself by signing up for the free, full-access, one-month trial with Quenza. You’ll be able to send out and complete all the forms you need.
Moreover, you’ll get access to everything that Quenza has to offer including a library of activities along with document management, scheduling, group functions and so much more. You’ll be providing tailored care that your clients will keep coming back for.
References
- ^ U.S. Department of Health and Human Services. (n.d.). Does HIPAA provide extra protections for mental health information compared with other health information? Retrieved from https://www.hhs.gov/hipaa/for-professionals/faq/2088/does-hipaa-provide-extra-protections-mental-health-information-compared-other-health.html.
- ^ Sutton, R. (2015). The Counselor's STEPS for Progress Notes: A Guide to Clinical Language and Documentation (2nd ed.). CreateSpace Publishing.
- ^ Borcherding, S., & Morreale, M. J. (2013). The OTA's Guide to Documentation (3rd ed.). Slack Incorporated.
- ^ Smith, C. M., Stavig, A., McCann, P., Moskovich, A. A., & Merwin, R. M. (2021). “Let’s talk about your note”: Using open notes as an acceptance and commitment therapy based intervention in Mental Health Care. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.704415.
- ^ Blease, C. R., O’Neill, S., Torus, J., & Walker, J. (2020). Sharing Clinical Notes in Psychotherapy: A New Tool to Strengthen Patient Autonomy. Front Psychiatry. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7655789/.
- ^ Guo, L. (n.d.). OLD CARTS History-taking Mnemonic. Osmosis from Elsevier. Retrieved from https://www.osmosis.org/answers/old-carts-history-taking-mnemonic.
I appreciate that you explained the importance of timely therapy solutions for an effective treatment process. My cousin told me the other day that he was hoping to find a psychotherapy treatment solution to help him boost his spiritual and mental health. He asked if I had any idea what would be the best option for a proper consultation. Thank you for the information on the importance of the proper treatment process.