Having a solid and consistent structure for writing your notes as a speech therapist comes with a range of benefits.
By using a tested format in your practice, like SOAP notes, you can cut down on administration time and improve the quality of care you provide. You’ll also be able to create defensible documentation you can confidently share with insurers, clients, parents, teachers, and other clinicians.
To help you become a master of documentation, we’re going to unpack several SOAP notes examples for speech therapy in this article. We’ll also provide some general tips for producing high-quality documentation and progress notes.
What are SOAP Notes in Speech Therapy?
SOAP notes are a standardized format for clinical documentation that’s used by all types of healthcare providers (such as occupational therapists, physiotherapists, physicians, speech therapists, counselors, and more) across the globe.[1]
The SOAP format includes 4 elements for a speech therapy progress note, identified by each letter in the acronym:
-
Subjective
This section usually frames the purpose of the session and the demeanor of the client.
It also lists any relevant background information, such as diagnoses, medical history, and current problems and goals. It captures all the subjective information shared by the client. -
Objective
Lists the concrete observations from the session.
Results from any testing, along with outcomes from activities and exercises are described here. As the heading suggests, this section is for recording data objectively and clearly by the speech therapist. -
Assessment
Provides your clinical assessment of the presenting situation.
Here you use your clinical reasoning to explain the significance of what was documented under the Subjective and Objective headings. This might include a diagnosis, comment on progress/goal attainment, or another form of professional opinion. -
Plan
Gives a clear indication of the next steps for all relevant parties.
The plan ensures there is a defined plan of action for the speech therapist, client, and anyone else involved in treatment. This might include more than one step, but shouldn’t project too far ahead into the future.
The Value-First Practitioner (Free Guide)
Discover how 10,000+ practitioners grow their practices through client transformation, not marketing.
Benefits of the SOAP Format
Following the SOAP format ensures that every speech therapy progress note you create contains all the necessary clinical information from a session. It also presents your documentation in a way that is familiar and easy to understand for non-speech therapist readers (e.g., parents, insurers, other clinicians).
Most importantly, however, is that SOAP notes can enhance the quality of care you provide by improving clinical reasoning and decision making.[2] This is because the structure ensures you address all important areas of patient care in each session, then finish with a clear plan.
To show you how to write SOAP notes for speech therapy, we’ll provide some speech SOAP note examples in the following section.
2 Speech Therapy SOAP Note Examples
You can write SOAP notes by hand or onto a blank electronic notes form. However, most clinicians find a template with headings easiest to work with.
Below, we’ve used the ready-made, customizable SOAP notes template from the Quenza app to give some speech therapy progress notes examples.
Patient #1111 FINCH, Jenny
This speech therapy SOAP note was created with Quenza’s drag-and-drop form builder:
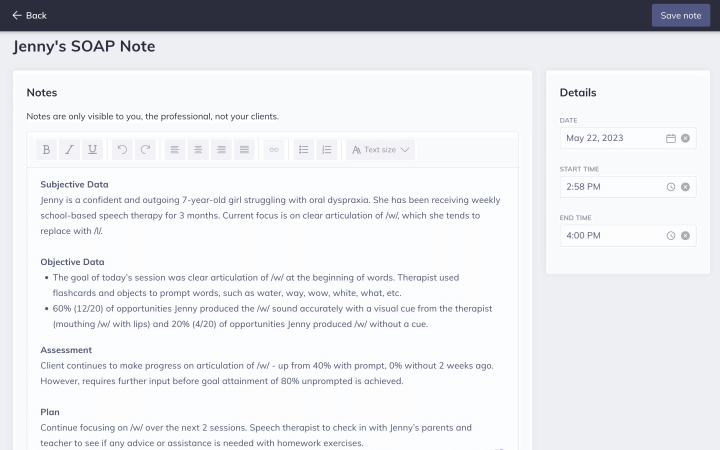
Quenza Notes automatically categorizes SOAP notes and other client documents according to time, date, and client.
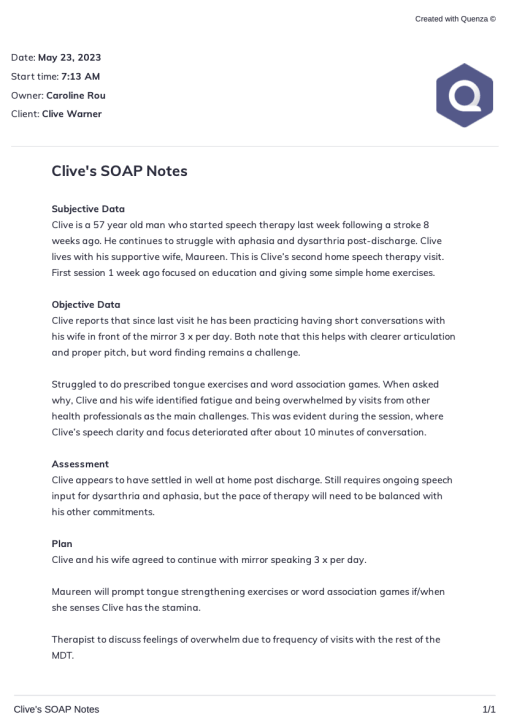
Patient #2222 WARNER, Clive
If you prefer to write notes by hand, you can even print out a blank SOAP notes template from Quenza and take it with you on home, school, or community visits.
Here’s a speech therapy SOAP notes example created with the Quenza printable PDF template:
How to Write Clearly & Efficiently with the SOAP Format
Two qualities speech therapists should strive for when writing SOAP notes are clarity and efficiency.
Clarity is important because it’s essential your notes are easily understood by others. And efficiency matters because spending longer than necessary on documentation means you’ll have less time to spend with patients.
Inefficient documentation processes can also increase the stress levels of clinicians, due to constantly feeling like you have to “catch up” on your notes.
To improve clarity:
- Stick to the headings
- Focus on the facts
- Don’t forget the plan
To document more efficiently:
- Use pre-made templates
- Go all-digital, using a speech therapy app
- Keep your audience in mind
5 Tips for Documenting Progress
The ideal processes for documentation will vary according to each speech therapist’s work setting and personal preferences.
For example, a therapist working in a busy hospital environment might need to approach documentation differently compared to someone in private practice. And a home visiting speech therapist will have different workflows to a practitioner completing all their therapy sessions online.
However, there are some tips for documentation that apply to the majority of speech therapists, which we’ll detail below.
- Write notes soon after the session – It’s best practice to write your speech therapy SOAP notes as soon as possible after the session. That way, the necessary information will be fresh in your mind. Plus, you won’t have to worry about falling behind on your documentation and getting stressed about having a bunch of unwritten notes.
- Use SMART plans – The SMART framework for goal setting (making goals Specific, Measurable, Attainable, Relevant, and Time-Based) can be very helpful when writing the Plan section of a SOAP note. This framework ensures that you provide clear and actionable next steps, without getting into ambiguous or irrelevant details.
- Link to other sessions – The best SOAP notes examples in speech therapy describe the current session in the context of the overall course of treatment. This might take the form of mentioning the previous session and how this one carries on from it. Or by commenting on the significance of the current session in relation to the patient’s progress so far.
- Stay consistent – Most speech therapists use acronyms and abbreviations in their SOAP notes. To ensure that others can understand your notes, it’s very important to be consistent in how you use technical and shorthand terms. For example, if a note uses “discharge” and “DC” interchangeably throughout, the reader may become confused about the meaning of the acronym. Choose one descriptor for each term and stick with it in all your notes.
- Remember the rest of the team – While the focus in most examples of SOAP notes for speech therapy is on the immediate session with the client, you’ll often need to mention other members of the team. The patient’s “team” might include their teacher, parents, other healthcare professionals, or even a partner or close friend.
Understanding the Legal and Ethical Implications of SOAP Notes
De use of SOAP notes in speech therapy not only improves clinical efficiency and quality of care but also has significant legal and ethical implications. Thorough and accurate documentation is crucial for defending against potential legal actions and ensuring compliance with regulatory requirements. Speech therapists must adhere to professional standards and guidelines, such as those set by the American Speech-Language-Hearing Association (ASHA), to maintain the integrity of their practice.
Ethical considerations include maintaining client confidentiality, obtaining informed consent for treatment, and ensuring that documentation is truthful and accurate. Inaccurate or incomplete SOAP notes can lead to misunderstandings, misdiagnoses, and potential harm to clients, which can have legal repercussions. Additionally, proper documentation supports transparency and accountability in clinical practice, fostering trust between therapists, clients, and other stakeholders.
By understanding and adhering to the legal and ethical standards of SOAP note documentation, speech therapists can protect themselves and their clients, while also contributing to the overall credibility and professionalism of the field.
Leveraging Technology for Efficient SOAP Note Documentation
Incorporating technology into the documentation process can significantly enhance the efficiency and effectiveness of SOAP notes in speech therapy. Various software solutions and applications are available that streamline the creation, storage, and sharing of clinical notes. These tools often come with templates, auto-fill features, and prompts that ensure all necessary information is captured accurately and consistently.
Additionally, digital SOAP notes can be easily updated, searched, and retrieved, saving valuable time for therapists. Cloud-based solutions provide the added benefit of secure access to notes from anywhere, facilitating collaboration with other healthcare providers and enabling more integrated care. The use of electronic health records (EHRs) also improves data accuracy and reduces the risk of errors associated with manual documentation.
Furthermore, technology can aid in the analysis of clinical data, helping therapists track progress over time, identify patterns, and make data-driven decisions. By leveraging technology, speech therapists can reduce administrative burdens, enhance the quality of their documentation, and ultimately improve client outcomes. Embracing digital tools not only modernizes the practice but also aligns with the broader healthcare industry’s shift towards more efficient and effective electronic documentation systems.
Final Thoughts
In this article, we’ve used SOAP notes examples for speech therapy to show you how to create high-quality notes quickly and efficiently.
Getting comfortable with the SOAP framework helps to cut down the time and effort required for documenting speech therapy sessions. It also ensures that every note you write contains all the essential information in an easy-to-understand format for your target audience.
To make documentation even easier, the Quenza app contains ready-to-use SOAP notes templates that you can print out and write by hand, or even complete directly in the app. All of our templates are completely customizable, allowing you to create your own “cheat sheet” to streamline documentation even further.

Start Your Free 30-Day Trial
Support your clients between sessions, where real change happens. Try Quenza free for 30 days and add up to 5 clients at no cost.
References
- ^ Wright, A., Sittig, D. F., McGowan, J., Ash, J. S., & Weed, L. L. (2014). Bringing science to medicine: an interview with Larry Weed, inventor of the problem-oriented medical record. Journal of the American Medical Informatics Association : JAMIA, 21(6), 964–968.
- ^ Podder, V., Lew, V., & Ghassemzadeh, S. (2021). SOAP notes. In StatPearls Internet. StatPearls Publishing.